2023.09.15
double-entry burial
The implantation method I employ

Dr Kuroda
Finally, the last session of the implantation method.
I didn't expect to go on for four weeks on the topic of implantation.
So far, we have given a bird's-eye view of the implantation method.
In this final installment, I will explain the implantation method I employ and why.
CONTENTS
Eyelid Lift or Eyelid Plate? Eyelidoplasty?
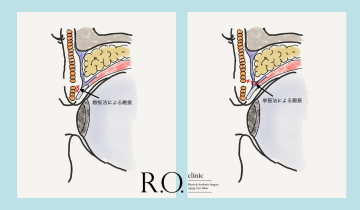
Basically, we use the "eyelid plate method" and also perform the raising muscle method when necessary. As explained in the previous two columns, there are advantages and disadvantages to both the eyelid plate technique and the elevator technique. Although I consider the raising muscle technique to be a very excellent method, I am concerned about the complication of eyelid spasm.
While the risks of the eyelid-plate technique, such as distortion of the eyelid plate and corneal damage, are complications that can be largely avoided if the surgery is performed with care, eyelid spasm is a concern because there is no sure way to avoid it. For this reason, we basically use the eyelid-plate technique.
There is no precise data on the risk of eyelid spasms occurring with the raising of the eyelid technique, but even if it is only a 1% chance, it will eventually happen if many surgeries are performed. I am a cautious type of person when it comes to surgery, so I try to perform as many surgeries as possible using the eyelid plate method.
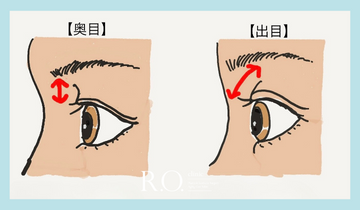
However, there are cases in which we dare to use the raising muscle method. The most common case is that of a patient who desires a wider double-exposed eye that is difficult to create with the eyelid-plate technique. If a patient with mongolian folds desires a parallel double-exposed eyelid, the eyelid plate near the top of the eye is tapered, so if this cannot be accommodated with the eyelid plate technique, only the top of the eye may be treated with the raising muscle technique. If the patient has already had a previous implantation at another clinic and the eyelid plate is already deformed, an elevator technique may be performed to prevent the deformation of the eyelid plate from worsening.
Point fixed? Loop fixed?
The "loop fixation" is used for threading. Point fixation is simpler as a technique, and if multiple threads are used for point fixation, it has the advantage of being less likely to come off from the targeted double design. However, I use loop fixation because threading the thread in a loop shape has the advantage of pulling the skin in with a surface and is less likely to come off than point fixation.
Front clasp? Back clasp?
The position of the thread ball is "front clasp" and not back clasp.
The back clamping is a method in which the thread is threaded from the conjunctival side and the thread ball comes to the conjunctival side. Many clinics use this method because it has the advantages of not leaving scars on the skin and the thread ball does not float. From the patient's point of view, it seems to have a lot of advantages, doesn't it?
I employ a table-top fastener for two reasons.
The first is that it is easy to remove the implantation threads when you want to remove them. If you are not satisfied with the double-layered line, or if you feel discomfort, you may need to remove the implantation thread. In such cases, if the threads are removed from the conjunctival side, the threads will be removed from the conjunctival side in principle. If the doctor is able to remove the thread with certainty, he/she may perform back clamping, but we do not perform back clamping because we believe it is difficult to remove the thread without damaging Müller's muscle.
Second, we do not believe that the thread ball is a bad actor to begin with. When removing a buried thread, we can see that the ball of thread is strongly adhered to the surrounding tissue. Once the ball of thread is found and removed from the surrounding tissue, the remaining thread can be smoothly removed. In other words, the thread ball is what keeps the implant from loosening and keeping the double fold in place. The ball of thread is a little bit pitiful, because it is hated by everyone, even though it supports the eye for thousands of blinks every day. We believe that if the ball of thread is at just the right depth subcutaneously, the double layer will last longer than if it is on the conjunctival side.
Of course, we do not think that thread balls should be noticeable even in the front fastening. I try to make the ball of thread as inconspicuous as possible. The more times the ball of thread is tied, the larger the ball of thread becomes. 3 to 5 times is often enough, but I use the method of tying 3 times to prevent it from unraveling. The thicker the skin, the less transparent the ball of thread will be, and the thinner the skin, the more transparent it will be. Usually, I use 7-0 threads, but if the skin is very thin and the thread ball is expected to stand out, I may use 8-0 threads, which are thinner. 7-0 threads are better at keeping the double-layer in place. However, people with thin skin have good retention of the double fold, so there is no problem with 8-0 threads.
Incidentally, the method of making multiple thread balls on a single thread is an excellent method in terms of fixation, but it is not simple to remove, so I use a single thread ball on a single implant.
How many stitches fixed?
The number of threads to be inserted ranges from one to three, depending on the thickness of the eyelid and the desired double fold shape. The more threads are inserted, the higher the price, so if clinic management is a priority, it is better to fix all patients with 3 stitches. However, even the implantable threads are foreign to the eyelids, so we try to propose the minimum number of threads necessary.
I am surprised and impressed by some clinics that offer expensive implantation to patients who clearly have a tendency to have a double-exposed eyelid, explaining that it is difficult for you to have a double-exposed eyelid, but I cannot in good conscience bear such upselling.
This concludes the series of columns on the implantation method.
Since the content has been somewhat difficult for the general public, I would like to make the next issue a little more relaxed and readable.
See you again in my next column.
Assistant Director Daiki Kuroda
# Dr. K's In-Depth Commentary Series
Supervisor of this article
vice president (of a hospital, clinic, etc.)
Daiki Kuroda
OHKI KURODA
Share Article