2024.11.15
double incision
Upper eyelid sagging excision
double-entry burial
Impact of implantation on double incision surgery

Dr Kuroda
It has been a long time since I have written a column.
CONTENTS
Does a history of implantation affect the double incision?
The theme of this year's event is
How does a previous eyelid implantation affect the ability to perform a bifid incision?"
It is.
The contents of this article are not intended for the general public, but rather for young doctors who are learning about eyelid surgery. We apologize for any inconvenience.
From the patient
How many implantations can I do?"
Do you find it harder to do a double incision if you have an implantation?"
It is a difficult subject, but if you are interested, please see this page.
Although implantation is a minimally invasive procedure, scarring still occurs under the skin.
In cases where the patient has undergone repeated implantation, the surgical operation becomes more difficult because of the strong scarring.
The effect on the eyelids varies depending on the implantation technique.
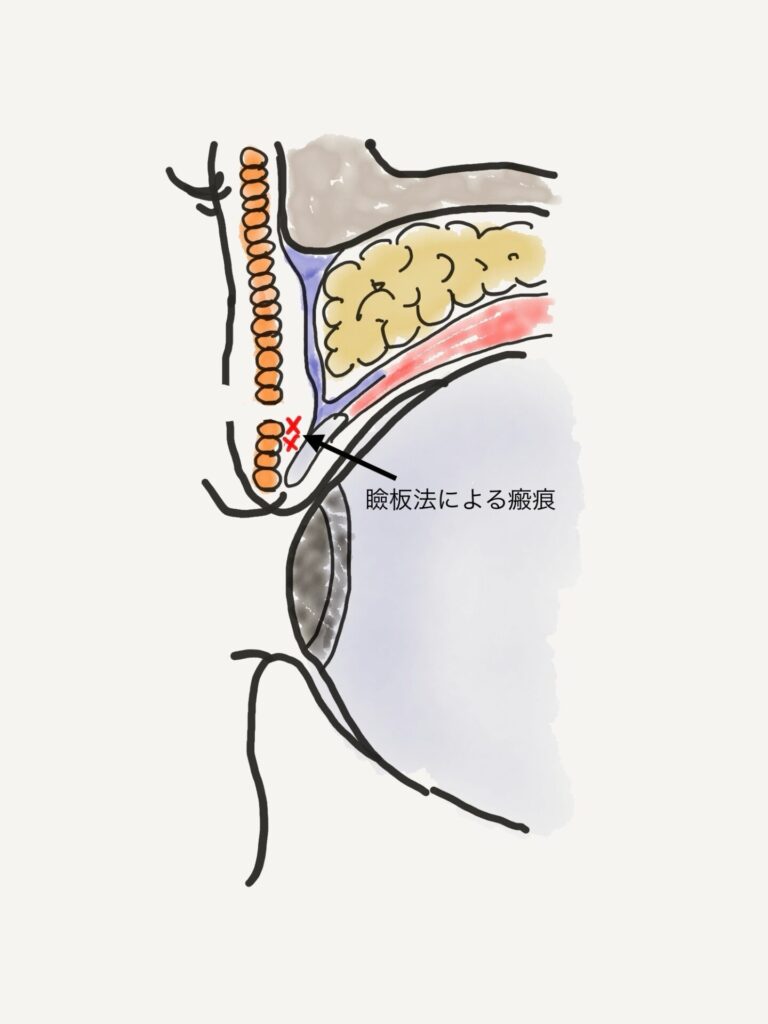
Blepharoplasty
There is an adhesion between the orbicularis oculi muscle and the tissue over the eyelid plate. With line or loop fixation, removal is easy, but with point fixation, the thread is often buried in the eyelid plate, and attempts to forcibly remove the thread risk loosening the connection between the eyelid plate and the levator tendon membrane, creating a droopy eyelid in the surgical manipulation.
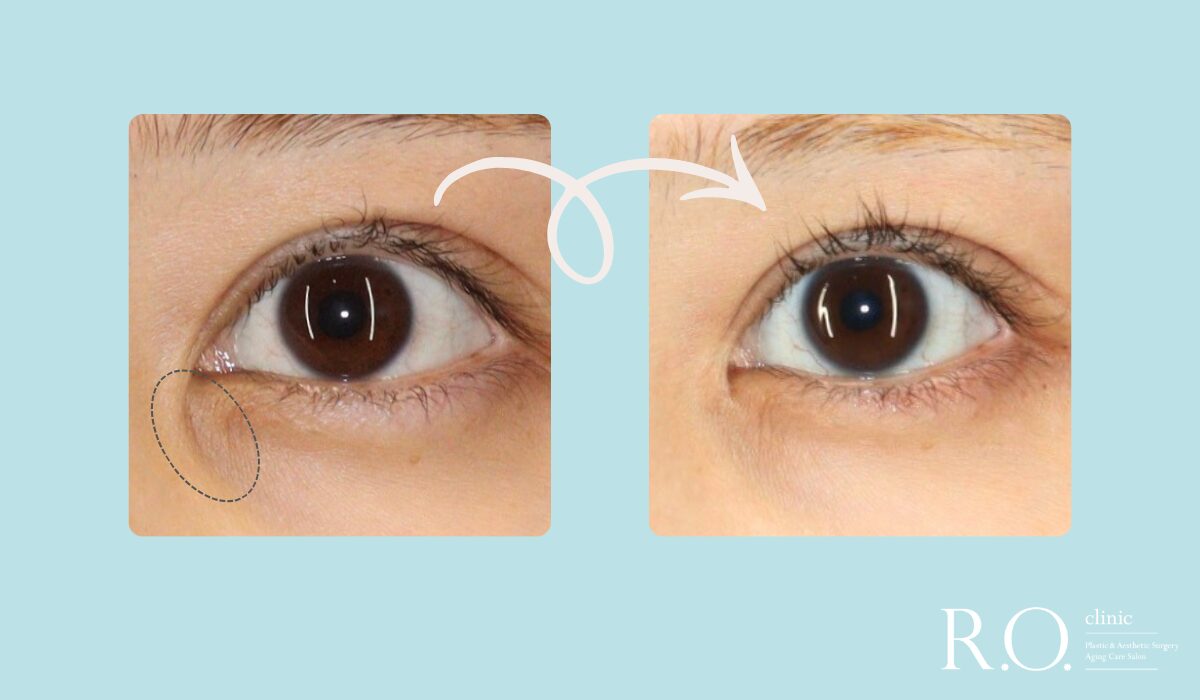
Threads that are buried without showing through the surface do not need to be forcibly removed, but they should be carefully removed if the eyelash line is hidden by the double-layer line created by the implantation technique.
To achieve a clean lash line, we want to pull the tissue over the lashes in toward the head, so the adhesion of the implanted threads on the eyelid plate will be resistant to this.
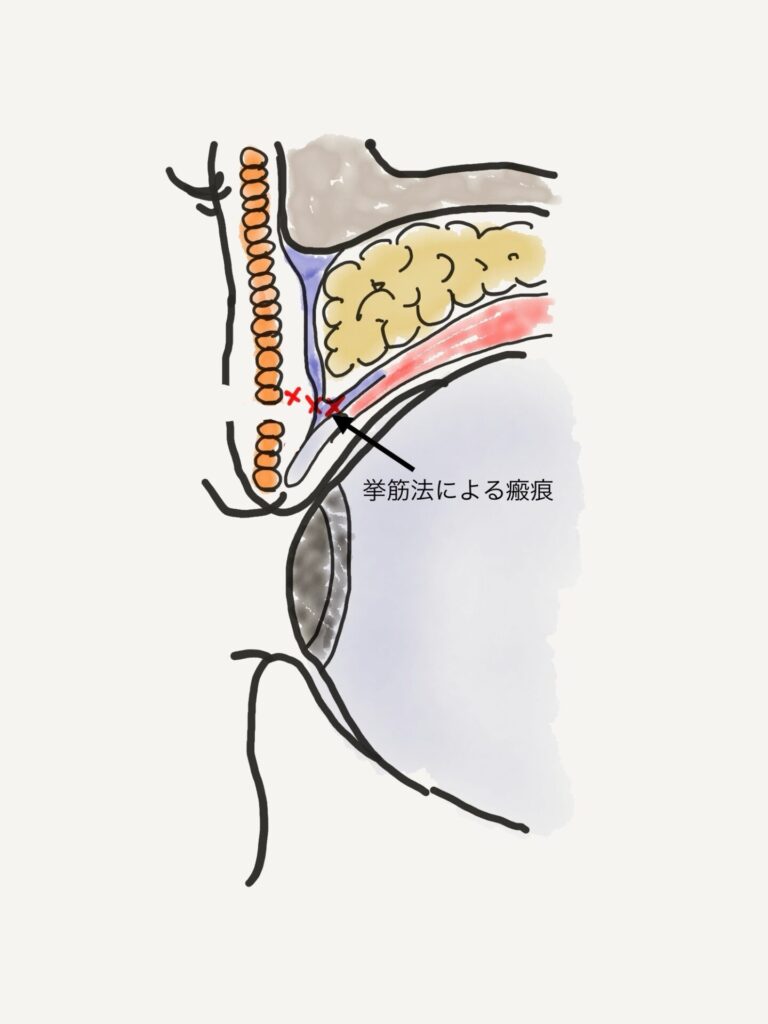
In the case of the elevator muscle method
In the elevator technique, the thread is loosely tied so that a long, loose thread remains under the skin. Therefore, it is relatively easy to find the thread when an incision is made. In some cases, it may be difficult to remove multiple knots of thread or multiple threads that are entangled in the technique.
In the case of raising the eyelid technique, adhesions may be created around the area where the orbital septum folds back from the tendon membrane of the levator tendon. If scarring is severe in this area, the source of heavy eyelid fixation is less flexible and may be more difficult to fine-tune when creating a heavy eyelid.
In cases where the double fold is not stabilized after multiple implantations and the incision is selected, the scarring from the raising of the orbital septum further increases the difficulty of the surgery because in many cases the orbital septum is thick with multiple layers or the inferior transverse ligament is developed, making tissue deployment difficult.
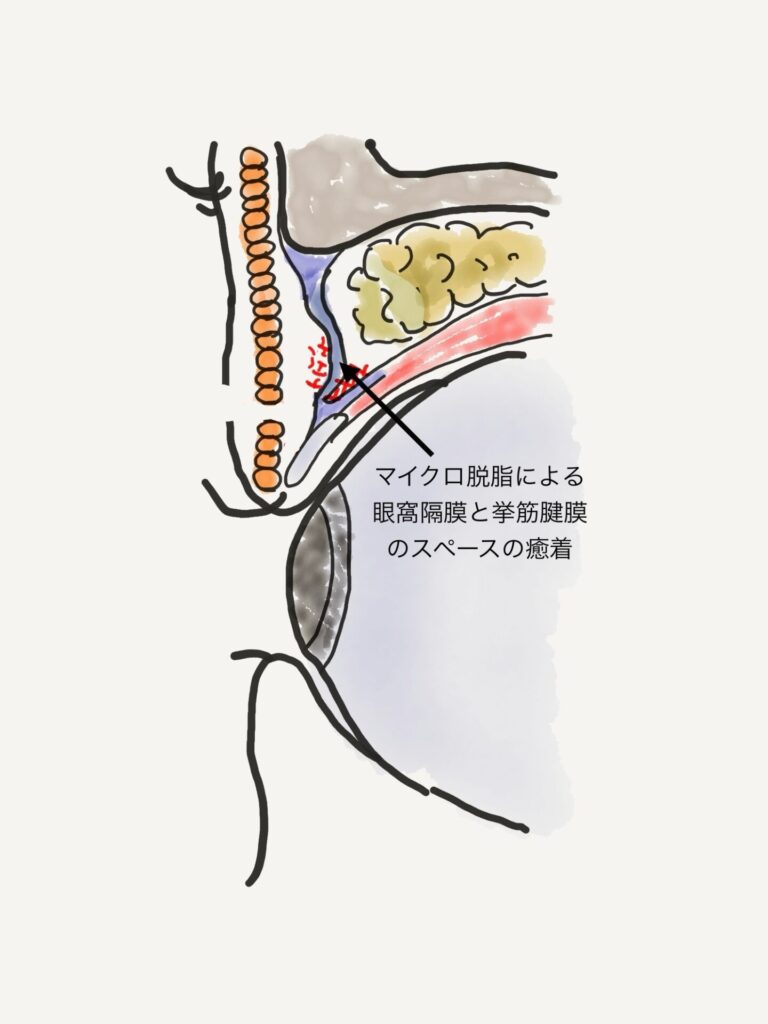
If you have microdebridement by implantation method
Normally, the orbital septum can be safely reached by opening the orbital septum while checking the orbital fat that can be seen through the orbital septum. However, the microdilated eyelids are more difficult to deploy due to the lack of orbital fat. If one is not familiar with the technique, it is difficult to distinguish the tissue and may damage the levator tendon membrane. Usually the outer orbital fat is more abundant, but in these cases the inner orbital fat is often left behind and easier to detect.
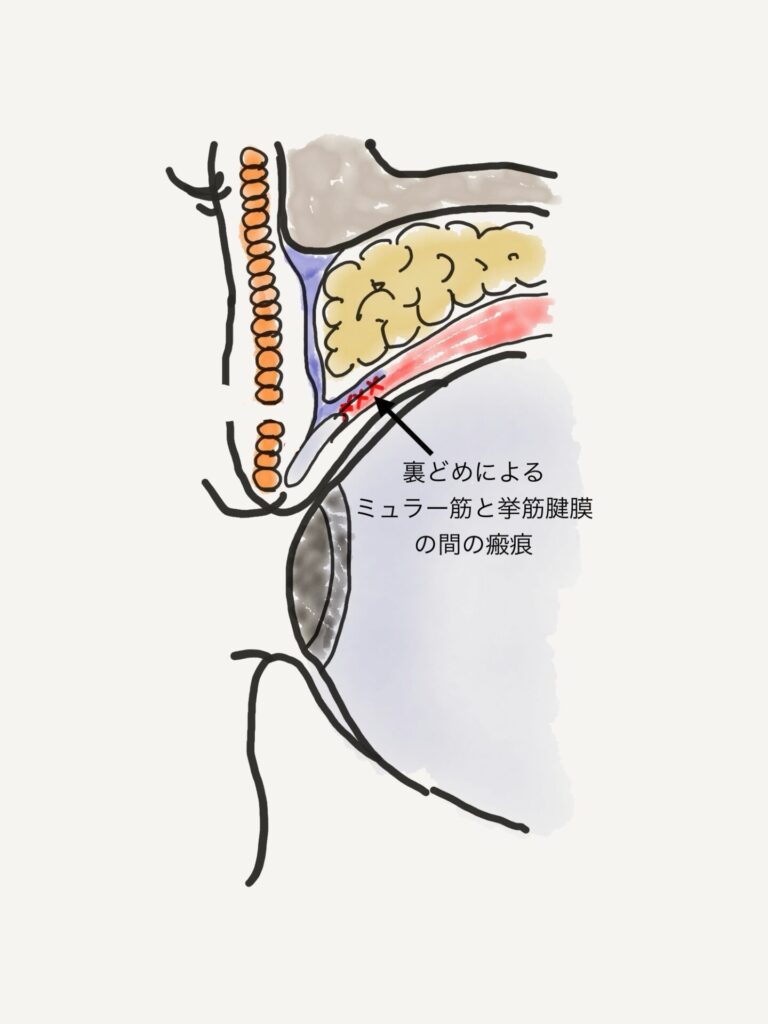
Cases that have been backfilled
The back-filled thread ball is buried around the Müller muscle. In the case of back-filling, the threads cannot be removed during the normal double incision process.
The most affected case of a backed-up eyelid is when performing ptosis surgery. It interferes with the dissection between the levator tendon and Müller's muscle.
Normally, the space between the glenohumeralis and Müller muscle can be smoothly developed by pulling the glenohumeralis tendon toward the patient while pulling the eyelid plate caudally. However, in the case of a backed-up blepharoplasty, it is more difficult to detach the levator tendon from Müller's muscle. In the process of detachment, a hole may be created in the levator tendon membrane, and swelling due to bleeding from the Müller muscle may make it difficult to adjust the eye opening.
What we ask patients during counseling
When I perform a double incision, I
How many times have you had a burial?
・Which clinic are you having the implantation procedure done at? (Because different clinics tend to have different subcutaneous scarring conditions.)
Is orbital fat removed during the implantation procedure?
We make every effort to accurately determine the patient's prior history of implantation, such as
We believe that by anticipating the effects of the implantation method while performing the surgical operation, we can perform the surgery more safely and smoothly.
Assistant Director Daiki Kuroda
#Dr. K's In-Depth Commentary Series
See details of the treatment related to ▼ column here.

Supervisor of this article
vice president (of a hospital, clinic, etc.)
Daiki Kuroda
OHKI KURODA
Share Article