2024.01.13
double incision
Internal processing of incisional double folds

Dr Kuroda
Rarely do patients ask for
How is the internal process handled in an incisional double?"
I read online that there are clinics that just cut and sew and don't do internal treatments, but is the doctor doing it right?"
They may ask questions such as.
If the discussion is between doctors, it can be explained smoothly because both parties have medical knowledge and a common understanding of the anatomy of the eyelid.
In the case of patients, we do not know how much knowledge they have, nor do we know how much detail they want to know, so we have a hard time explaining.
I recently had the opportunity to receive a similar question in a counseling session, so I will explain it in my column.
Although we have used illustrations to help the reader understand visually, the content is rather technical and should only be read by those who are interested in the subject matter.
CONTENTS
Introduction: Upper Eyelid Anatomy
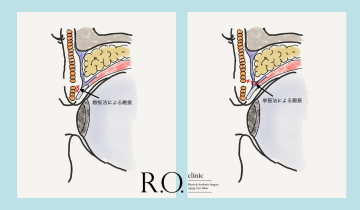
First is an illustration of the anatomy of the upper eyelid. It is simplified for the general public.

The purpose of bifid surgery is to create a bypass that transfers the force of the eyelid elevator muscle, which is drawn along the eyeball when the eyelid is opened, to the skin.
Explanation of Internal Processing
Now, let us follow the surgical process.
Skin incision - orbicularis oculi incision
A scalpel is used to make the skin incision. There are also laser and electrocautery incisions, but I am a scalpel person because I do not like to create burns on the edges of the wound. It is shorter to make the incision all the way to the orbicularis oculus at once, but I only make the skin incision so as not to scar the orbicularis oculus. The orbicularis oculi muscle has many blood vessels on its surface, so I stop the bleeding of those vessels first and then make the incision in the orbicularis oculi muscle. Since blood vessels also run within the orbicularis oculus, when making an incision in the orbicularis oculus, we make the incision little by little to stop the blood vessels from bleeding before making the incision. We believe that by carefully performing this process, internal bleeding and swelling after surgery will be minimized.
Subcutaneous peeling, removal of implanted threads, orbicularis oculi procedure
A peel is applied just below the orbicularis oculi muscle to the eyelash side. If there are any implantation threads present during this process, they are removed as much as possible. For those who have had implantation, there is adhesion between the anterior eyelid tissue and the orbicularis oculi muscle, so all of this adhesion is also removed to allow smooth movement of the tissue on the eyelash side. The orbicularis oculi muscle on the eyelash side is preserved as much as possible. Although removing the orbicularis oculi muscle creates a firm double fold that does not loosen easily, it also has the disadvantage of creating a floppy double fold with little movement and making revision surgery more difficult. In the case of a patient who has difficulty in forming a double fold when a bougie double fold is simulated, an appropriate amount of the orbicularis oculi muscle is removed.

Opening and reversal of the orbital septum
The orbital septum is inverted through an incision on the brow side of the skin incision. The orbital septa should be expanded well to the lateral and lateral edge of the eye, as a half-open orbital septa will cause resistance to eyelid opening. It is important to prepare an inverted orbital septum that is long enough to allow smooth transmission of the eyelid elevator muscle movement.

Eyelid Opening Resistance Treatment
The inferior transverse trabecular ligament restrains the eyelid elevator tendon membrane from above. This inferior transverse ligament varies greatly from person to person, but if it is well developed, it is removed because it interferes with the movement to open the eye.
If the implantation is performed with an elevator technique or if the upper eyelid has undergone a blepharoplasty, there may be cobweb-like scar tissue between the orbital fat and the tendon membrane of the levator tendon. Since this webbed tissue interferes with the movement of the eye opening, the area between the orbital fat and the levator tendon is also thoroughly debrided to allow smooth movement of the levator tendon.
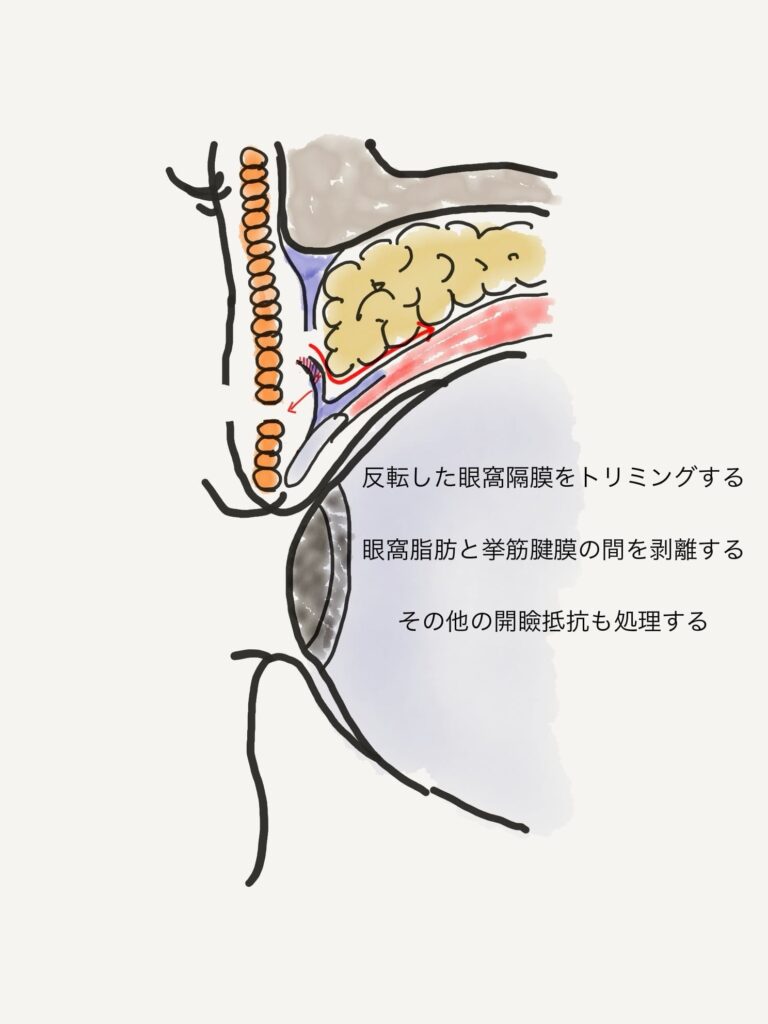
double-edged eyelid fixation
Adjust the orbital septum that has just been inverted by resecting it to the appropriate length.
By inverting the orbital septum long enough, it is possible to resect the orbital septum and to some extent the ROOF at the same time. Three to five subcutaneous fixations are made on the inverted orbital septum and the eyelash side using absorbable thread. The internal process of heavy eyelid fixation includes fixation to the eyelid plate, to the anterior tissues of the eyelid plate, or to the tendon membrane of the eyelid elevator muscles. The method that I employ, using the inverted orbital septum as the fixation source, has the advantage of providing a more natural result with less bite at eyelid closure. On the other hand, there are some risks associated with this method, such as the difficulty in adjusting the width of the bifocal fold and the possibility of loosening the fixation of the heavy eyelid. The appropriate length of the orbital septa to use for fixation of the heavy eyelid can only be learned through experience with many surgeries.

skin graft
Finally, the skin is stitched together with nylon thread, scooping out the inverted orbital septa in places. For patients with thin skin and concave eyes, orbital fat may be pulled out during the skin suture to prevent the appearance of an unscheduled eyelid line.

The methods described in this article are general methods for initial surgery. In the case of a revision from another clinic or when creating an extremely wide or narrow double fold, the method of fixation of the eyelid may be changed.
Finally.
This column is intended for patients who do not feel comfortable without knowing all the details.
Just as you can board an airplane and reach your destination without knowing why the plane is flying, you do not need to know how to perform the internal double-overlap procedure in order to achieve the desired double-overlap, so please rest assured that we will perform the surgery with appropriate internal processing.
Assistant Director Daiki Kuroda
#: Dr. K's In-Depth Commentary Series
See details of the treatment related to ▼ column here.

Supervisor of this article
vice president (of a hospital, clinic, etc.)
Daiki Kuroda
OHKI KURODA
Share Article