2023.12.29
correcting a hangnail
About Hanging Eye Correction

Dr Kuroda
The theme of this issue is about one of my popular treatments, "Hanging Eye Correction".
I mentioned it briefly in a previous column, but I will provide a more thorough and in-depth explanation.
*Reference column:What's the difference between suspension correction and glamorous line formation?
CONTENTS
What is suspension correction?
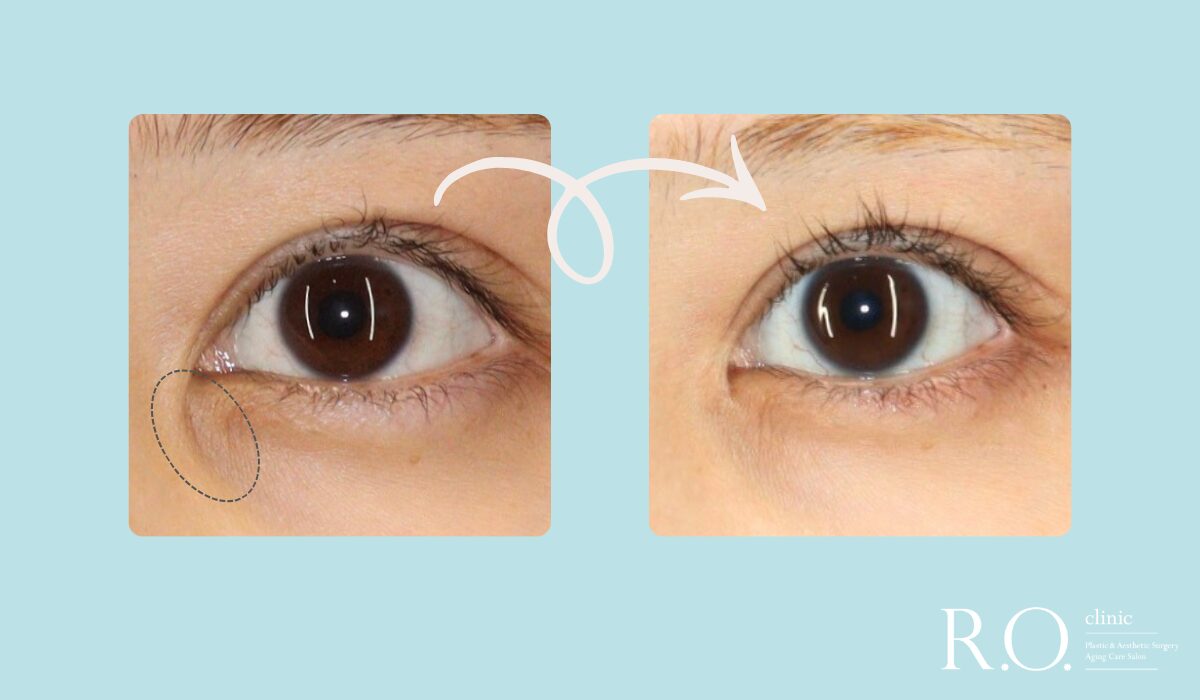
This surgery, as the name implies, improves the impression of a hanging eye by lowering the outer corner of the eye outward and downward. In other clinics, the same technique may be called "lower eyelid control surgery" or "Tare eye lid incision". It is possible to lower the position of the outer corner of the eye without making the lower eyelid arch convex downward as in glamorous lines or tale eye formation. Since the position of the outer corner of the eye is lowered diagonally outward, it also has the effect of enlarging the eye in the lateral direction, as in the case of an incision at the outer corner of the eye. Seeing is believing, so let's take a quick look at actual case photos.



You can see that the outer corner of the eye has dropped outward and downward, and the outer whites of the eyes have become larger.
What kind of surgery?
The position of the eye socket is determined by where the ligaments attach to the bone. If you gently touch the inner corner of the eye with your fingertips, you will feel a stiff, immobile tissue at the back of the eye. That is the ligament. The ligament at the corner of the eye is located slightly deeper and cannot be touched unless you press your finger in strongly (do not try to touch it, as it is dangerous).
During surgery, a skin incision of a few millimeters is made at the corner of the eye and a portion of the ligament that supports the lower eyelid is detached. Once the ligament is detached, the lower eyelid becomes wobbly and is re-fixed around the bone in just the right position, which is the outline of the suspension correction.
I have been performing this technique since 2018 and feel that there are various tricks to it, such as ligament fixation sites, tissue to leave, tissue to excise, and skin incision design. The details of the tricks are too geeky for the general public, so if you are interested, please ask me in a consultation.
About Downtime
Surgery can be performed under local anesthesia alone, but for those who are more anxious, surgery is performed under laughing gas or intravenous anesthesia. Stitches are removed 7 to 10 days later. If the sutured thread is short, it will prickle, so it is left a little longer and fixed to the skin with tape. If I use a softer thread, I can cut the suture shorter and omit the tape fixation, but I feel that the finish is more beautiful if I use nylon thread, so I currently use nylon thread.
Because the corner of the eye is an area with many blood vessels, it is not uncommon for internal hemorrhagic spots to occur. Some people may experience conjunctival edema, a jelly-like swelling of the whites of the eyes. This is temporary and usually improves in about two weeks.
Let's take a look at the downtime of suspension correction.

Immediately after surgery, the eye is lowered so firmly that it becomes a lower trinocular. The thread is fixed to the skin with tape placed at the corner of the eye.

This is the condition of the patient immediately after the stitches were removed one week later. This patient has minimal internal hemorrhage spots and no conjunctival edema. The first week immediately after surgery is the period when retroversion occurs the most.

This is the state after 1 month. The redness at the corner of the eye has gone down, and there is almost no regression after one month.

Before and after. The impression of the hanging eyes has been softened and the eyes have been enlarged.
See also another patient with internal hemorrhagic spots and conjunctival edema one week postoperatively.
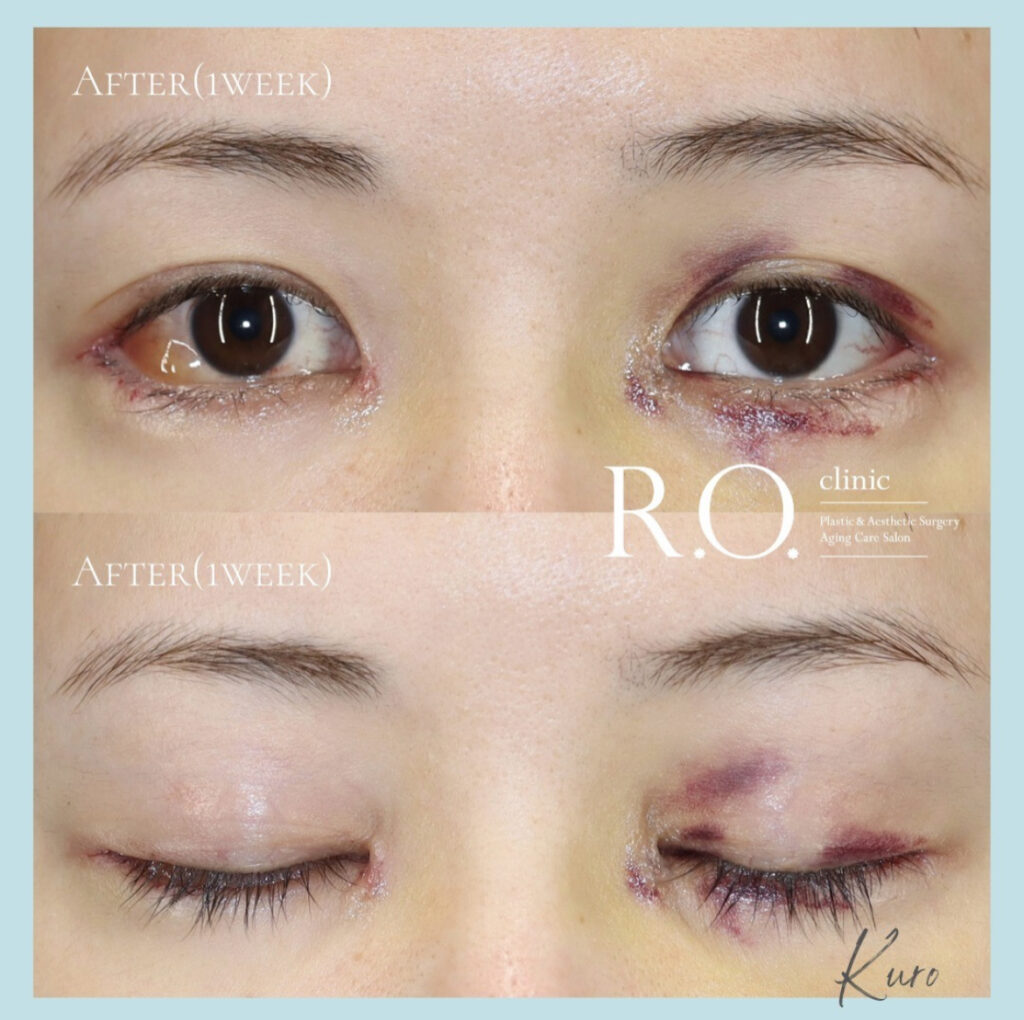
Conjunctival edema is present in the corner of the right eye. The left eye has a more intense internal hemorrhagic spot.
Thus, even if the same surgeon performs the surgery, it is inevitable that there will be differences in the degree of downtime.
Effect on double width
Only the ligaments connecting to the lower eyelid are separated and re-fixed, while the ligaments connecting to the upper eyelid are preserved. As you can see from the case photos, there is virtually no effect on the shape of the double fold.
complications (in an illness)
The most frequent problem is the left-right difference in the height of the outer corner of the eyes. People who have no difference in the original position of the outer corner of their eyes can align the height of their eyes quite accurately, but people who have a difference in the original height of the outer corner of their eyes will find it difficult to align it completely. This is because the skeletal structure to which the ligaments are attached also differs between the left and right eye lids of those who originally had a left-right difference.
Have a doctor who is familiar with the procedure perform the suspension correction.
We have seen cases in other hospitals where the conjunctiva at the corner of the eye is heavily exposed or the lower eyelid is puckering away from the eyeball due to an excessive skin cut or an error in the ligament fixation site.
This technique is a surgery with many detailed tricks. One must be familiar with the length of skin that can be safely incised based on the depth of the pocket in the corner of the eye, a three-dimensional understanding of the area where the ligament is to be reattached, how to leave tissue to stabilize the ligament reattachment, and how to treat the orbicularis oculus muscle to reduce retroversion to achieve a stable result.
Since this is still a minor surgery compared to double-layer surgery or craniotomy, we believe that some experience is necessary to achieve consistent results.
This column is photo-heavy, but I will end with a monitored case study of a combination of popular procedures at our clinic.

This is a patient who underwent both the Hanging Eye Correction and the Mongolian Fold Formation VY method at the same time. By lowering the outer corner of the eyes and rounding the inner corner of the eyes, the patient's eyes became gentle as if she were a different person.
Thank you for reading to the end.
Deputy Director: Hiroki Kuroda
#Dr. K's In-Depth Commentary Series
Supervisor of this article
vice president (of a hospital, clinic, etc.)
Daiki Kuroda
OHKI KURODA
Share Article